

Duchenne muscular dystrophy and its causes?
It is a hereditary disease transmitted by women to their male descendants. Although Duchenne muscular dystrophy has no cure, advances in treatments have improved patients’ quality and life expectancy.
Duchenne muscular dystrophy (DMD) is a genetic disease caused by a shortage or total lack of a protein called dystrophin, responsible for the proper functioning of muscle contraction. It is the most common myopathy (muscle disease) in children. Another dystrophinopathy is considered a “minor form” of it, called Becker’s dystrophy, with a later onset and with milder symptoms, but with the exact origin in terms of little or no dystrophin production.
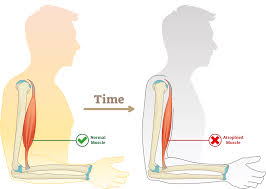
This type of dystrophy was described for the first time in France by Dr. Duchenne in 1860. It usually appears in children between two and six years old. It is characterized by a progressive and rapid evolution that causes the muscles to weaken to the point that, over time, the patient loses the ability to walk and has respiratory and heart problems. Characteristically, in the early stages of the disease, there is an increase in the calf muscles’ size, but due to the deposition of fat and fibrous tissue (pseudohypertrophy).
The cardiac and pulmonary disorders are the main cause why these children die around the second or third decade of life because they develop heart disease and the high rate of bronchopulmonary infections sufferers.
It is a genetic disease, with an incidence of a male between 3,600-6,000 live births linked to the X chromosome. Therefore it is usually only suffered by men and will only be transmitted by women.
Although there is currently no curative treatment for Duchenne disease despite some open clinical trials, the main objective is muscle physiotherapy to try to offer better mobility and independence to the patient and avoid as much as possible his cardiopulmonary complications over the years life of these patients.
The Duchenne muscular dystrophy is a disease of genetic origin; the gene responsible for the disease is recessive and linked to the X chromosome, so women do not usually have symptoms (in their case, the genetic abnormality of one of the X chromosomes is compensated by the other X chromosome, which is normal). Still, they do transmit it to male children through the defective chromosome. Male children of female carriers have a 50% chance of suffering from the disease, while daughters have a 50% chance of being carriers.
When a patient is diagnosed with the disease, it is observed that:
- In one-third of the cases, a clear family history of the disease is collected.
- In one-third, muscle changes are observed in the mothers of affected patients, and the mutation is considered maternal.
- In a third, no family member with a muscle disorder is identified, and it is considered a mutation of the patient.
As for the genetic cause itself of Duchenne muscular dystrophy, several models of mutations have been detected in the DYS gene (responsible for this process). On the one hand, there is the possibility that they are deletions, which are losses of some fragment of the DNA of the gene responsible for the production of dystrophin. On the other hand, they can be duplications of said gene, and approximately 20% are point mutations in some sequence of the gene’s DNA.
These disorders unbalance the structure of the gene, losing the dystrophin production function, totally or partially. This protein would bind under normal conditions (glycoprotein), forming a complex responsible for muscle contraction. By altering this process, muscle cells break down in the contractions that cause creatine kinase to be released into the blood (a substance that is detected in tests).





